When a cough lasts longer than eight weeks, it’s not just annoying-it’s a signal that something deeper is going on. Most people assume it’s just a lingering cold or allergies, but if it won’t go away, the real culprits are often three hidden conditions: GERD, asthma, and upper airway cough syndrome (formerly called postnasal drip). Together, these three cause 80 to 95% of chronic cough cases in adults who don’t smoke or take blood pressure meds like ACE inhibitors. The good news? You don’t need a dozen tests to find out what’s causing it. A smart, step-by-step approach can get you answers in weeks-not years.
Start with the basics: what your history and exam tell you
Before any scans or blood tests, your doctor should ask you the right questions. Not just, "How long have you been coughing?" but: Does it wake you up at night? Does it get worse after meals or when you lie down? Do you feel a lump in your throat or need to clear it often? Have you started a new medication recently? These details matter. A cough that shows up after eating or at bedtime? That’s classic GERD. One that flares up around pollen season or after exercise? Likely asthma. Constant throat clearing with a runny nose? That’s upper airway cough syndrome. A physical exam isn’t just a formality. Listening to your lungs can reveal wheezing (a red flag for asthma) or silence where there should be air movement. Checking for swollen nasal passages or mucus dripping down the back of your throat helps confirm UACS. And don’t skip the chest X-ray. It’s quick, cheap, and rules out serious stuff like lung cancer or tuberculosis. If your X-ray is normal-which it usually is-you’re already in the right ballpark.Rule out the obvious: medications and red flags
Before chasing down GERD or asthma, you need to eliminate the easy stuff. Are you taking an ACE inhibitor? Drugs like lisinopril or enalapril cause cough in up to 35% of users. The cough usually starts within a week to six months of starting the pill. Switching to a different blood pressure med can make the cough vanish in days. That’s one of the few quick fixes in chronic cough. Then there are the red flags. If you’re coughing up blood, losing weight without trying, running fevers, or have swelling in your legs, you’re not dealing with the "big three." Those symptoms demand faster, deeper testing-like a CT scan or biopsy. But if you’re otherwise healthy and just have a persistent cough? You’re likely dealing with one of the three common causes.Testing for asthma: it’s not always wheezing
Asthma doesn’t always come with wheezing. In fact, about one in four cases of chronic cough are caused by what’s called cough-variant asthma-where cough is the only symptom. Spirometry, a simple breathing test, is the first step. If it’s normal, that doesn’t rule out asthma. The real test? A bronchodilator challenge. You breathe in a medicine that opens your airways, then repeat the test. If your lung function improves by at least 12% and 200 milliliters, asthma is likely. Another option is a methacholine challenge: you inhale a mist that triggers airway tightening. If your lungs react strongly at low doses, you have hyperresponsive airways-classic asthma. Treatment? Inhaled steroids and bronchodilators. Most people feel better in two to four weeks. But here’s the catch: if you’re misdiagnosed, you’ll keep coughing. That’s why the test matters. You can’t just guess.
GERD: the silent cough culprit
GERD is tricky because most people with GERD-related cough don’t have heartburn. Up to 70% of these patients never feel acid rising. It’s called silent reflux. Stomach acid travels up the esophagus and irritates the throat, triggering a cough reflex. That’s why treating it isn’t as simple as popping a Tums. The old way? Give you a high-dose proton pump inhibitor (PPI) like omeprazole twice a day for four to eight weeks. But here’s the problem: only half to three-quarters of people respond. And guess what? About 40% of people who don’t have GERD still feel better on PPIs because of placebo effect. That’s why the American College of Gastroenterology updated its guidelines in March 2024: Don’t start PPIs without evidence. If your cough doesn’t improve after a proper trial, it’s probably not GERD. Newer tools help. The Hull Airway Reflux Questionnaire (HARQ) scores symptoms like throat clearing, hoarseness, and post-meal cough. A score above 13 suggests laryngopharyngeal reflux with 80% accuracy. For stubborn cases, a 24-hour pH impedance test measures acid in the esophagus and throat. But it’s expensive, and insurance often won’t cover it unless you’ve tried the basics first.Upper airway cough syndrome: the most treatable cause
This is where the old term "postnasal drip" falls short. It’s not just mucus dripping down. It’s a hypersensitive cough reflex triggered by inflammation in the nose and throat. Allergies, colds, pollution, or even dry air can set it off. The good news? This one responds best to treatment. The diagnostic test? A trial of first-generation antihistamines (like brompheniramine) plus a decongestant (pseudoephedrine) for two to three weeks. No CT scans. No nasal sprays. Just this combo. If your cough drops by 70 to 90%, you’ve got UACS. Most people notice improvement within a week. Side effects? Drowsiness, dry mouth-but that’s why first-gen antihistamines work better than newer ones like loratadine. They cross the blood-brain barrier and calm the cough reflex directly. Newer guidelines now call it "upper airway cough syndrome" because it’s not about drainage-it’s about nerve sensitivity. Treat the nerves, not the mucus.The diagnostic algorithm: what order matters
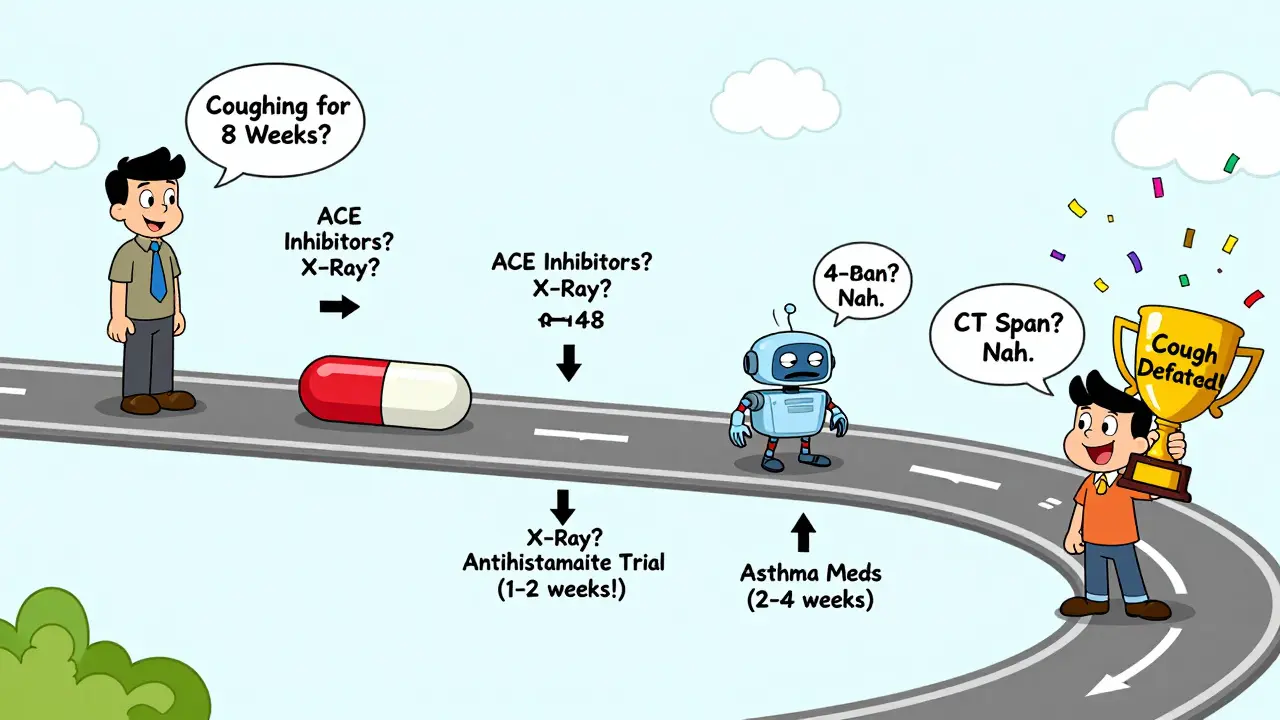
There’s a reason doctors don’t start with a CT scan. The sequence matters. Here’s what works:- Rule out ACE inhibitors and red flags.
- Do a chest X-ray and spirometry.
- Try treatment for UACS first-it has the highest success rate (70-90%).
- If that fails, try asthma treatment (inhaled steroids + bronchodilator).
- If still no improvement, try a PPI trial for GERD.
- If none work? Look at rarer causes: chronic aspiration, pertussis, or chronic refractory cough.
Why so many people get it wrong
Doctors often prescribe antibiotics for chronic cough. That’s a mistake. Less than 5% of cases are caused by bacterial infections like pertussis. And even then, you need a special nasal swab to detect it-it doesn’t show up on regular tests. Another problem? Placebo effect. People feel better on any treatment, even if it’s not the right one. That’s why a proper trial with clear timelines matters. UACS: 1-2 weeks. Asthma: 2-4 weeks. GERD: 4-8 weeks. If you stop after a week, you’ll never know if it worked. And then there’s the cost. A 24-hour pH test can run over $1,000. Insurance often requires prior authorization. That’s why many primary care doctors stick to the trial-and-error method. It’s practical. It’s low-risk. And when done right, it works.What’s next? New tools on the horizon
In 2022, the FDA approved gefapixant, the first drug specifically for chronic refractory cough. It blocks a nerve signal that makes you cough. In trials, it cut cough frequency by 18-22%. A newer drug, camlipixant, showed even better results in 2024-24.7% reduction versus placebo. AI is stepping in too. A 2023 study in Lancet Digital Health trained a machine to listen to cough sounds. It could tell asthma cough from GERD cough with 87% accuracy. Imagine a phone app that analyzes your cough at home. That’s not science fiction anymore. The European Respiratory Society now recommends the Hull Cough Questionnaire to measure how much your cough affects your life. A score over 15 means your quality of life is seriously damaged. That’s when you know it’s time to act.What to do if you’ve been coughing for months
If you’ve been living with a cough for over eight weeks, here’s what to ask your doctor:- Have I been on any ACE inhibitors? If so, can I switch?
- Can we do a chest X-ray and spirometry?
- Can we try a two-week trial of an antihistamine plus decongestant?
- If that doesn’t work, can we try an inhaled steroid for asthma?
- If still no change, can we try a four-week PPI trial?
Can chronic cough be caused by something other than GERD, asthma, or postnasal drip?
Yes, but it’s rare. About 10-30% of chronic cough cases don’t respond to treatment for the "big three." Other causes include chronic aspiration (inhaling food or saliva into the lungs), pertussis (whooping cough), side effects from certain medications, or chronic refractory cough (a condition where the cough reflex becomes overly sensitive with no clear trigger). If you’ve tried all standard treatments and still cough, further testing-like a swallow study, bronchoscopy, or cough reflex sensitivity test-may be needed.
Why do some people get better on PPIs even if they don’t have GERD?
About 35-40% of people who take PPIs for chronic cough feel better-even if they don’t have acid reflux. This is called the placebo effect. The act of taking a pill, combined with the belief that it will help, can reduce coughing. It’s not just in their head-it’s a real neurological response. That’s why doctors now avoid starting PPIs without evidence. If you don’t have typical reflux symptoms and your cough doesn’t improve after eight weeks on PPIs, it’s likely not GERD.
Is a chest CT scan necessary for chronic cough?
No-not if your chest X-ray is normal. A CT scan exposes you to radiation equivalent to 74 chest X-rays, and it finds cancer in only 0.1% of cases with normal X-rays. Guidelines from the European Lung Foundation and ACCP recommend skipping CT scans unless you have red flags like weight loss, coughing up blood, or abnormal lung sounds. Start with the basics: history, exam, X-ray, and spirometry. Don’t jump to expensive scans.
Why do antihistamines help with postnasal drip if they dry up mucus?
It’s not about drying mucus. First-generation antihistamines (like brompheniramine) cross the blood-brain barrier and directly calm the cough reflex in the brainstem. That’s why they work better than newer ones like cetirizine or loratadine, which don’t affect the central nervous system. The decongestant helps reduce nasal swelling, which lowers irritation. Together, they target the nerve sensitivity that triggers the cough-not just the mucus.
How long should I wait to see if my treatment is working?
Timing matters. For upper airway cough syndrome, improvement usually happens in 1-2 weeks. For asthma, expect to wait 2-4 weeks for inhaled steroids to take full effect. GERD-related cough can take 4-8 weeks to respond to PPIs. If you stop treatment too soon, you’ll never know if it worked. Stick to the timeline. And if you don’t improve after all three trials, your doctor should consider rarer causes.

Aisling Maguire
February 28, 2026I’ve had this cough for 14 months. Tried everything-antihistamines, PPIs, inhalers. Nothing. Then I switched my pillow to a wedge and stopped eating after 7 PM. Cough vanished in 3 days. No one talks about sleep position. It’s wild how much gravity matters.
Also, stop drinking wine if you’re a nighttime crier. Acid doesn’t care if you’re "healthy."
Byron Duvall
March 1, 2026They’re all lying. This is all a Big Pharma scam. PPIs don’t work because they’re designed to keep you hooked. The real cure? Apple cider vinegar and cold showers. I’ve been cough-free since 2019. They don’t want you to know this. Why? Because pills = profit. Look up the FDA whistleblower reports. They buried it.
Full Scale Webmaster
March 2, 2026Okay but let’s be real-this whole "step-by-step" thing is a joke. I’m a nurse. I’ve seen 12 patients in the last 6 months with normal X-rays and spirometry who had silent reflux, asthma, and UACS all at once. They were misdiagnosed because doctors are lazy. They don’t want to do the work. So they give you a PPI and say "come back in 8 weeks."
Meanwhile, your cough is wrecking your sleep, your job, your relationships. I had a patient who lost her job because she couldn’t stop coughing during Zoom calls. They gave her Zyrtec. ZYRTEC. Like she had hay fever. She had esophageal dysmotility. Took 18 months and a $2000 pH test to figure it out.
And now they’re talking about AI cough analysis? That’s not innovation. That’s a Band-Aid on a hemorrhage. We need systemic change, not apps. Stop treating symptoms and start treating the nervous system. The vagus nerve is the real villain here. Not mucus. Not acid. Not allergens. NERVE HYPERSENSITIVITY. Read the 2024 Lancet paper on neurogenic inflammation. They’re still ignoring it.
Lisa Fremder
March 3, 2026Why are we letting foreigners tell us how to treat our own bodies? This "Hull Questionnaire"? Sounds like some EU nonsense. We have real American doctors who know what’s up. PPIs work. Period. If you’re not getting better you’re just not trying hard enough. I’ve been on omeprazole for 5 years and I’m fine. Stop overcomplicating everything. America built this country on common sense not fancy tests.
Justin Ransburg
March 4, 2026This is one of the most well-researched and clinically grounded summaries of chronic cough I’ve seen in years. Thank you for clearly outlining the diagnostic algorithm and emphasizing evidence-based sequencing. Too often, patients are subjected to unnecessary imaging and polypharmacy when a simple, structured trial could resolve their symptoms. The point about placebo response in PPI trials is particularly crucial-many clinicians overlook how powerful expectation effects can be in functional disorders. Your emphasis on timeline adherence is spot-on. Patients need to be educated that healing isn’t instant. This deserves to be shared widely in primary care circles.
Vikas Meshram
March 5, 2026There is a grammatical error in your paragraph on UACS. You wrote "first-generation antihistamines (like brompheniramine) plus a decongestant (pseudoephedrine) for two to three weeks." The correct term is "brompheniramine" not "brompheniramine." Also, the phrase "cross the blood-brain barrier" should be followed by a comma. Furthermore, the European Respiratory Society recommends the Hull Cough Questionnaire, not "Hull Airway Reflux Questionnaire." Please correct these inaccuracies. Misinformation in medical content is dangerous.
Ben Estella
March 5, 2026They’re all just playing the system. PPIs? Placebo. Antihistamines? Placebo. Even the "cough reflex" nonsense? That’s just a cover for Big Pharma’s real agenda: keep you on meds forever. You think they want you cured? No. They want you on a subscription. I know people who work in pharma. They laugh about this stuff. They call it "the cough economy." You think your doctor cares? He’s got a quota. I’ve seen the emails. This whole post? It’s a Trojan horse. The real cure? Fasting. Cold exposure. No sugar. No meds. Just primal living. But you won’t hear that from a university hospital.
Angel Wolfe
March 6, 2026They’re covering up the truth. The real cause of chronic cough? 5G towers. I live near a cell site. My cough started the day they installed it. I’ve got neighbors with the same thing. The government knows. That’s why they don’t test for it. The FDA approved gefapixant? That’s not a cure. That’s a distraction. They’re using drugs to keep people quiet while the radiation keeps building. You think they care about your cough? They care about your data. Your cough patterns. Your sleep. Your breathing. All tracked. All sold. Read the 2023 NDAA bill. Section 7.3. It’s all there. You’re being monitored. And now they want you to use a phone app? That’s the trap. Don’t fall for it.
Charity Hanson
March 8, 2026Y’all need to stop overthinking this. My cousin in Lagos had a cough for 10 months. Took her 3 days to fix it. She drank ginger-honey-lemon tea every morning. Ate papaya. Slept with her head up. No pills. No tests. Just food and rest. Africa doesn’t have fancy labs but we know how to heal. Stop chasing tests. Start healing. Your body is smarter than your doctor’s algorithm.
Sumit Mohan Saxena
March 9, 2026While the diagnostic algorithm presented is largely aligned with current clinical guidelines, I would like to emphasize the importance of distinguishing between idiopathic chronic cough and neurogenic cough. The 2023 ERS guidelines suggest that patients with refractory cough and normal structural findings on high-resolution CT should undergo quantitative cough monitoring using ambulatory cough-recording devices prior to initiating pharmacotherapy. Furthermore, the use of first-generation antihistamines should be approached with caution in elderly patients due to anticholinergic burden and risk of delirium. The recommendation for pseudoephedrine may also be contraindicated in patients with hypertension or cardiac arrhythmias. A comprehensive risk-benefit analysis remains essential, even within a stepwise approach.